
Most shoulder impingement is subacromial pain. The tendons of the rotator cuff, and the small fluid-filled sac that sits above them, get compressed and irritated in the narrow space beneath the bony point at the top of the shoulder. It usually shows up when you lift your arm to shoulder height or reach overhead, and it eases when you bring the arm back down.
It is one of the more common shoulder complaints the clinic team sees, and it is also one of the most misunderstood. The word “impingement” makes it sound like a purely mechanical trap that needs to be surgically opened up. For most people that is not what is going on, and it is not what the treatment needs to be.
The short version
- Impingement means the rotator cuff tendons are compressed under the shoulder blade.
- Pain is worst reaching overhead or out to the side.
- It is usually a tendon-load problem, not a structural trap.
- Progressive exercise is the first-line treatment, not surgery.
- See a GP urgently for trauma, fever, or arm weakness.
What is actually being impinged
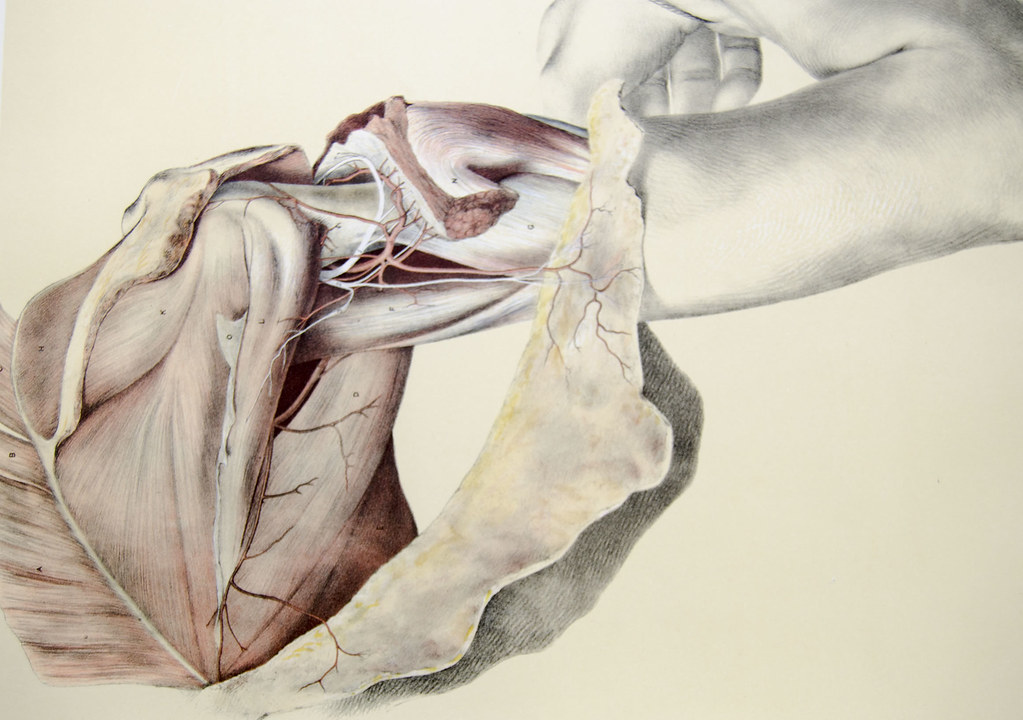
The rotator cuff is a group of four muscles whose tendons wrap around the top of the arm bone and hold the ball of the shoulder centred in its socket. Above those tendons sits the acromion, the bony shelf you can feel as the tip of your shoulder, and between the two sits the subacromial bursa, a thin sac that lets the tendons glide.
When people say “impingement” they usually mean subacromial pain, sometimes called subacromial pain syndrome. The tendon of the supraspinatus muscle and the bursa become irritated and swollen in that subacromial space, so movements that narrow the space, reaching up and out, pinch and hurt. The pain is often felt on the outside of the upper arm rather than on the top of the shoulder itself.
The older idea was that the shape of the acromion was mechanically trapping the tendon, and that shaving the bone would solve it. The evidence has moved on. In most cases the tendon is irritated because of how it has been loaded, not because it is being physically crushed by bone.
Why it starts
The common thread is a change in load the tendon was not ready for. That might be a new job with a lot of overhead reaching, a return to swimming or racket sport after a layoff, a decorating weekend, or a gym programme that added overhead pressing too quickly. The tendon protests, swells slightly, and then every overhead movement aggravates it.
Age plays a part too. Rotator cuff tendons lose some of their tolerance from the forties onwards, so the same task that was fine at thirty can tip into pain at fifty. Posture and desk work get blamed a lot, and while a permanently rounded position does not help, it is rarely the whole story on its own. The load history matters more than the posture snapshot.
In the years I was practising, the pattern I saw most was not a single injury. It was someone who had gradually done more overhead work than usual over a few weeks and could not point to one moment it started.
What tends to help, and what does not
The first-line treatment is progressive exercise that gradually rebuilds the tendon’s tolerance, usually starting below the painful range and building up. A Cochrane review of manual therapy and exercise for rotator cuff disease found exercise helps function, though it was honest that the quality of the evidence is low and the size of the benefit is modest. The Chartered Society of Physiotherapy also lists graded exercise and staying active as the mainstay for most shoulder pain.
Hands-on treatment, including the soft-tissue and joint work an osteopath does, can help settle symptoms and improve how the shoulder moves in the short term, which often makes the exercises easier to do. It works best alongside a loading programme rather than instead of one. On its own, passive treatment tends to help less and for less time.
What tends to disappoint people is waiting it out with rest alone. Complete rest lets the tendon quieten but does not rebuild its tolerance, so the pain often returns as soon as normal activity resumes. Steroid injections can reduce pain for a while and are sometimes useful to get a stalled rehab moving, but they do not fix the underlying load problem.
Surgery has moved down the list for good reason. A large placebo-controlled trial, the CSAW trial published in The Lancet, found that keyhole surgery to shave the bone was no better than a placebo operation, and neither was clearly better than no surgery. For most subacromial pain, that is strong evidence to try loading and time first. Recovery is often slow, measured in months rather than weeks, and it tends to improve steadily rather than in one jump.
When to see a GP urgently
Most impingement is not an emergency, but some shoulder pain needs faster attention. Per NHS guidance on shoulder pain, see a GP urgently or seek same-day care if any of the following apply.
- A recent significant injury, especially with an obvious change in the shape of the joint or an inability to move the arm at all.
- The shoulder is hot, red, or swollen, or you feel feverish and unwell, which can point to infection.
- New weakness, numbness, or pins and needles down the arm or into the hand.
- Pain with tightness or pressure in the chest, or pain spreading to the jaw or left arm, which needs emergency care by calling 999.
- Unexplained weight loss, or a history of cancer, alongside new shoulder pain.
How we assess it
A proper assessment is about ruling things in and out, not guessing. The osteopath goes through your history, watches how the shoulder moves, tests the rotator cuff and the surrounding joints, and checks the neck, because neck problems can refer pain to the shoulder and mimic impingement. That tells us whether this is a straightforward loading problem or something that needs imaging or an onward referral. An initial assessment at the clinic is 45 minutes and costs £75, with follow-ups at £60.
Shoulder pain that is stubborn is often just a tendon that has been loaded wrong and then either rested too much or pushed too hard. A clear plan usually helps more than another few weeks of hoping it settles. If you want to understand a related shoulder problem that behaves very differently, our piece on frozen shoulder and its timeline covers a condition that is often confused with impingement.
If this sounds like what you are dealing with, an assessment is the next step. Book at hardimanperformance.com/book-online.