
Pelvic girdle pain in pregnancy is pain felt around the pubic bone, the hips, the groin or the lower back, caused by the way the pelvic joints move and carry load as pregnancy progresses. It affects roughly one in five pregnant women. It is common, it responds to treatment, and in most cases it settles after the baby arrives.
That last point matters, because a lot of women are told pelvic girdle pain is just something to put up with until birth. It is not. There is plenty you can do to make day to day life easier, and the evidence supports staying active rather than resting up.
The short version
- Pelvic girdle pain affects around 1 in 5 pregnant women.
- It comes from altered movement and load through the pelvic joints, not damage.
- It usually settles in the weeks after birth.
- Staying active within comfortable limits helps more than resting.
- Severe pain, bleeding, fever or reduced baby movements need urgent maternity review.
What pelvic girdle pain actually is
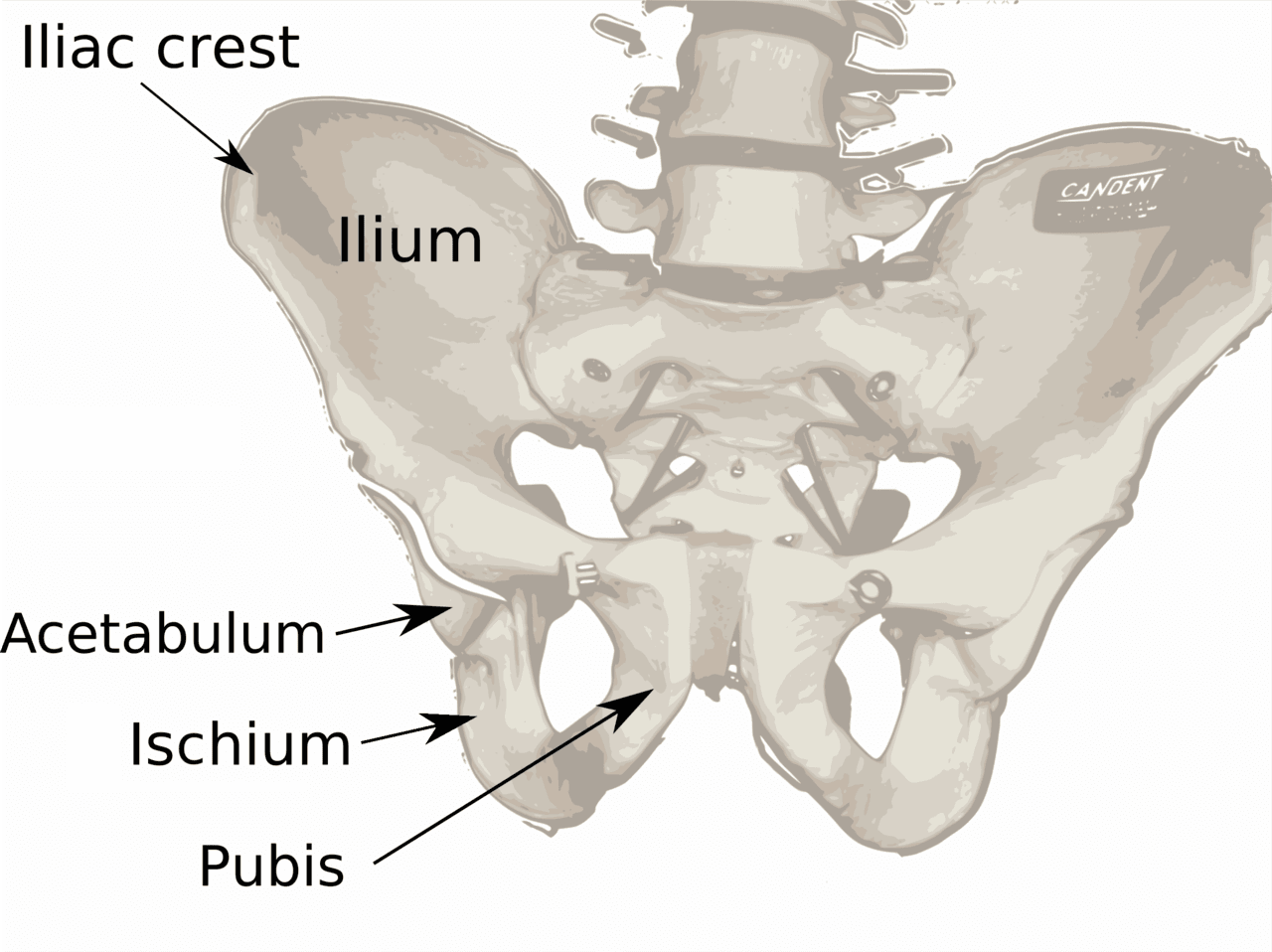
Pelvic girdle pain, sometimes still called symphysis pubis dysfunction, is the term for pain in the joints that make up the pelvic ring. That includes the joint at the front, where the two halves of the pelvis meet at the pubic bone, and the two joints at the back, where the pelvis meets the base of the spine.
The pain is usually felt at the front over the pubic bone, in the groin, across the lower back, or deep in the buttock. Many women notice it most when they part their legs, turn over in bed, climb stairs, or stand on one leg to get dressed. The NHS describes the same pattern, and it is one of the more reliable ways to tell pelvic girdle pain apart from ordinary pregnancy back pain.
Why it happens
Two things change during pregnancy and both load the pelvis differently. The first is hormonal. The body produces hormones that make ligaments more pliable to allow the pelvis to adapt for birth. The second is mechanical. As the bump grows, the centre of gravity shifts forward and the muscles that control the pelvis have to work in a new pattern.
The result is that the pelvic joints move slightly differently under load, and the surrounding muscles can become irritated and protective. It is worth being clear about one thing: pelvic girdle pain is a problem of how the joints are moving and being controlled, not a sign that the pelvis is damaged or coming apart. The Royal College of Obstetricians and Gynaecologists makes the same point in its patient guidance.
What tends to help
The general principle is to keep moving within the range that does not flare your pain, and to reduce the specific movements that aggravate it. In clinic, the things that tend to make the biggest difference are simple and practical.
- Keep your knees together when turning in bed, getting in and out of the car, and standing up. Moving the legs symmetrically loads the front joint far less.
- Take stairs one at a time, or lead with the less painful leg.
- Sit down to dress. Standing on one leg to put on trousers is one of the most common triggers.
- Pace your day. Pain that is fine in the morning and worse by evening usually means the load needs spreading out, not stopping.
- Gentle targeted exercise. Work that helps the deep abdominal and pelvic floor muscles support the pelvis tends to help, ideally guided by someone who has assessed you.
A supportive pelvic belt helps some women, particularly for walking and standing, though it is not a fix on its own. NICE antenatal care guidance (NG201) supports offering an exercise based approach and access to manual therapy where it is needed, rather than leaving women to manage alone.
What tends to make it worse
Some everyday habits quietly keep pelvic girdle pain going. Standing for long stretches with your weight on one hip, crossing your legs, pushing through a long shopping trip, and heavy lifting all tend to provoke it. So does staying completely still for too long, which is why bed rest is no longer advised for this. The aim is steady, comfortable movement, not avoidance.
When to get checked urgently
Pelvic girdle pain itself is not dangerous, but pregnancy brings a few situations that always warrant a faster route than a routine appointment. Contact your midwife or maternity unit straight away if you have vaginal bleeding, a sudden gush or trickle of fluid, a fever, or reduced movements from your baby.
Separately, certain nerve related symptoms need urgent medical assessment whether you are pregnant or not: numbness around the saddle area between the legs, loss of control of your bladder or bowel, or new weakness in the legs. These are uncommon, but they should never be filed under normal pregnancy aches. When in doubt, get it looked at.
How osteopathy fits in
Osteopathy for pelvic girdle pain is hands on work to ease the muscles and improve how the pelvic joints are moving and being controlled, alongside clear advice on positions and activity. Treatment during pregnancy is gentle and adapted to your stage, and a good session is as much about giving you a plan for the week as the time on the table.
I will be honest about the evidence here, because the brand of honesty matters more than the sale. The research on manual therapy for pelvic girdle pain is mixed, and no approach works for everyone. What the evidence does support consistently is staying active, individualised exercise, and reassurance, all of which we build into treatment rather than treating the hands on work as the whole answer.
If your low back or pelvis has been struggling and you want it assessed properly, our short guide on the first days of low back pain is a useful companion read.
If this sounds like what you are dealing with, an assessment is the next step. Book at hardimanperformance.com/book-online.