
Pain on the outside of the knee that comes on at a predictable point in a run is, in most active people, iliotibial band syndrome. It is the commonest cause of lateral knee pain in runners and cyclists. It is an overload problem in the soft tissue, not a sign that the joint itself is damaged, and it usually settles once the load on the tissue is managed properly.
The short version
- ITB syndrome is the most common cause of outer-knee pain in runners.
- It is a tissue overload problem, not joint damage.
- Pain typically starts at a fairly consistent distance or time into a run.
- Stretching the band on its own rarely fixes it.
- Managing load and building hip and knee strength is what works.
What ITB syndrome actually is
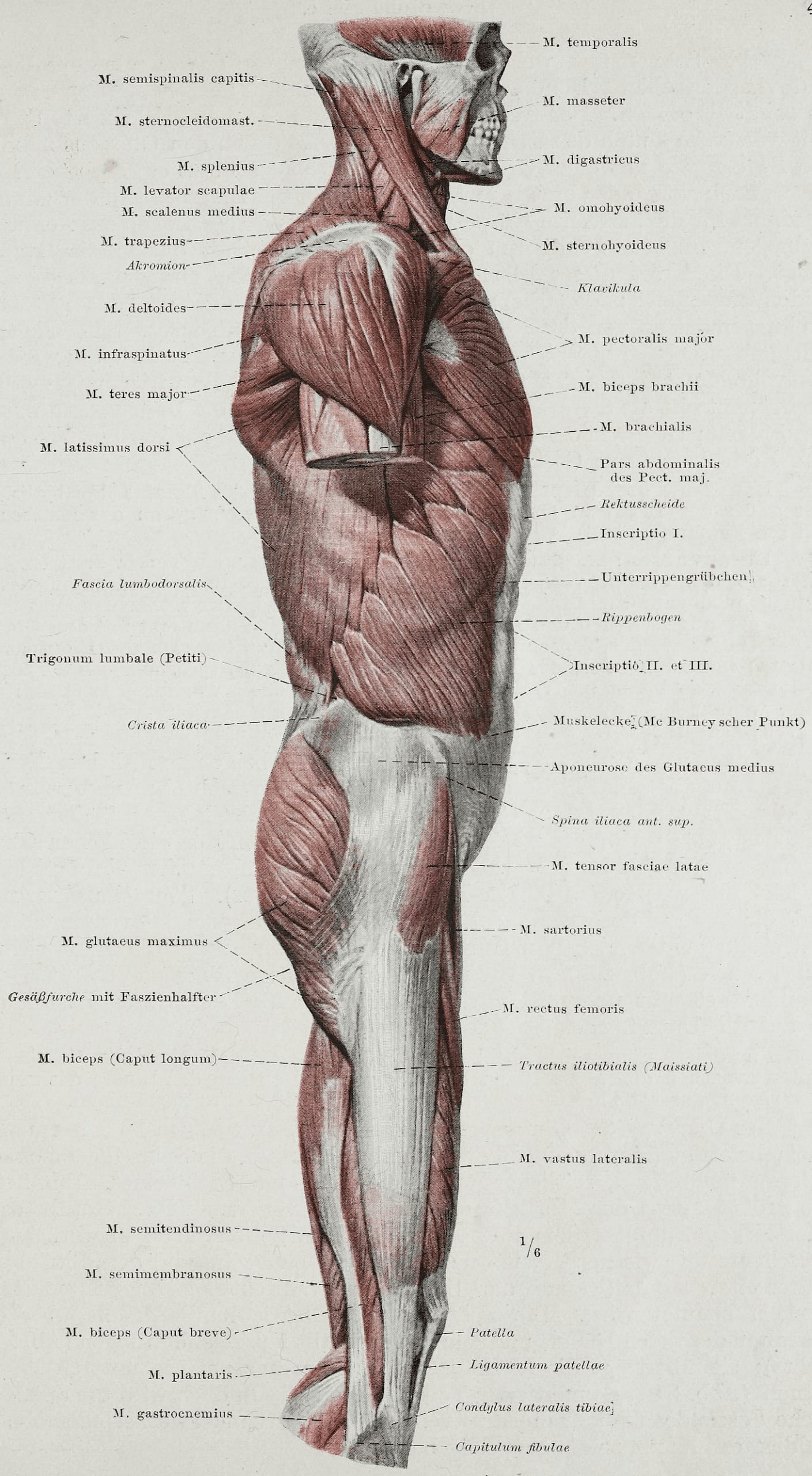
The iliotibial band is a thick strip of connective tissue that runs down the outside of the thigh, from the hip to just below the knee. Near the knee it passes over a bony bump on the outer edge of the thigh bone, the lateral femoral epicondyle.
When the knee bends and straightens repeatedly under load, the band and the sensitive fat pad beneath it get compressed against that bump. Do that often enough, with not enough recovery in between, and the tissue becomes irritated and painful. That is the whole mechanism. There is no joint to put back in place and nothing is slipping out of position. It is a load-versus-capacity problem, and that is good news, because load and capacity are both things you can change.
How to tell it is ITB syndrome and not something else
The pattern is usually quite recognisable. The pain sits on the outside of the knee, often sharp or burning, and it tends to come on at a fairly consistent point in a run. Many people can tell you the distance almost to the kilometre. It often feels worse running downhill or at a slower, more bent-knee cadence, and it eases with rest only to return at the same point next time.
That picture is different from the other common knee complaints. Pain right at the front of the knee or around the kneecap points more towards patellofemoral pain. Pain along the joint line with swelling, locking or giving way points towards the cartilage or the meniscus and needs assessing properly. Working out which structure is driving the pain is the first job of any decent assessment, and the UK clinical guidance on assessing knee pain follows the same logic.
It also helps to know who tends to get it. ITB syndrome usually turns up after a change in load rather than out of nowhere. A sudden jump in weekly mileage, a new block of hill work, returning to running after a break, or a switch to a harder running surface are the usual triggers. If you can pin down what changed in the two or three weeks before the pain started, you are usually looking at the cause.
When to see a GP or get urgent help
Most outer-knee pain in active people is a soft-tissue overload and is not dangerous, but a few signs warrant getting it looked at sooner. See a GP if your knee pain does not improve within a few weeks. In many parts of the UK you can refer yourself to an NHS musculoskeletal service without going through a GP first.
Get urgent advice from NHS 111 if your knee is very painful, you cannot put any weight on it, it is badly swollen or has changed shape, it locks or gives way, or you have a high temperature with redness and heat around the joint, which can be a sign of infection. The NHS page on knee pain sets out the same red flags. These are uncommon with ITB syndrome, but they are worth knowing.
What actually helps, and what does not
Load management is the centre of treatment. In the irritable early phase that usually means cutting back the aggravating load for a period, the downhill running and the long high-mileage sessions in particular, rather than stopping everything. Total rest tends to calm the pain down and then let it come straight back once running resumes, because nothing has changed about the tissue’s capacity to cope.
Building strength in the hip and the muscles that control the knee is the part that tends to hold the result. Stretching the band itself is the thing most people reach for first, and on its own it is the weakest tool in the box. You cannot meaningfully lengthen the iliotibial band by pulling on it, and stretching does little to change the compression at the knee. In the early painful days, an ice pack for up to twenty minutes and a short course of paracetamol or ibuprofen can take the edge off while the loading plan does the real work.
The return to full running is best done in steps rather than in one go. Once the knee tolerates easy, flat running without flaring up, mileage and then hills go back in gradually, watching how the knee responds over the following day or two rather than just during the run. Small changes to how you run can help too. A slightly quicker, shorter stride tends to reduce the load through the outside of the knee for some people. None of this is a quick fix, but it is reliable, and most people get back to the running they want to do.
What an assessment looks like
A first appointment is mostly working out why the tissue got overloaded in the first place. We watch how you move and run, test the strength and control around the hip and knee, and go through what changed before the pain started, whether that was a jump in mileage, a new training block, more hill work or a change of shoes. Treatment combines hands-on work to settle the irritated tissue with a graded loading plan you can actually follow.
The aim is to get you running again with a plan, not to hand you a list of stretches and tell you to stop. An initial assessment is £75. If you want to read more about how we handle running and sport complaints, our sports injury clinic page covers what to expect.
If this sounds like what you are dealing with, an assessment is the next step. Book at hardimanperformance.com/book-online.