
A disc bulge and a disc herniation are not the same thing, but for most back pain neither finding on its own explains the pain. A bulge is a disc spreading slightly beyond its normal border. A herniation is the soft inner core pushing through the outer wall. Both are common in people who have no back pain at all.
If you have just been handed an MRI report with one of these words on it, the wording can sound alarming. The job of this post is to translate it. What the terms actually mean, why the report rarely matches how much pain you feel, and when a disc problem is genuinely worth acting on.
The short version
- A disc bulge is broad and mild. A herniation pushes further through the outer wall.
- Both show up routinely on scans of people with no pain.
- The words on your report rarely match how much it hurts.
- Most disc-related back pain and sciatica settle over weeks to months.
- See a GP urgently for numbness around the saddle area or bladder changes.
The plain-English difference
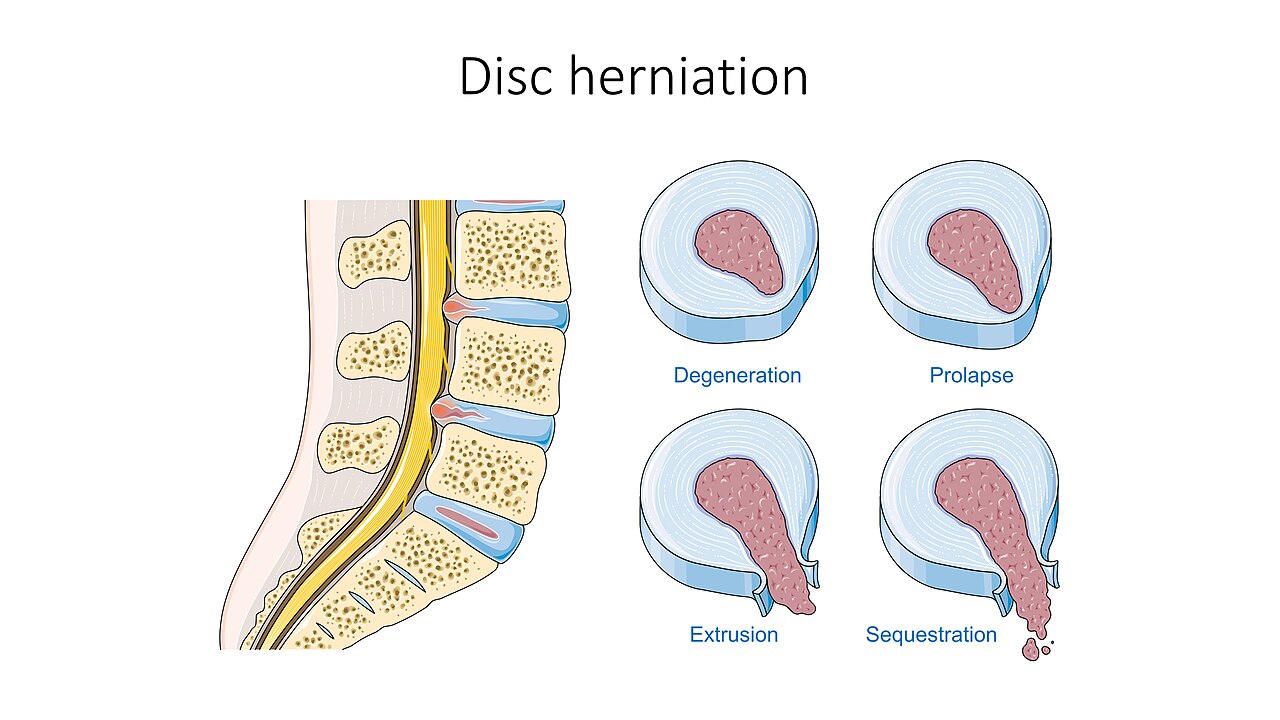
An intervertebral disc sits between each pair of spinal bones. It has a tough outer ring, the annulus, and a soft gel-like centre, the nucleus. The disc works as a spacer and a shock absorber, and it lets the spine bend and rotate.
A disc bulge is when the disc spreads out beyond its normal edge in a broad, even way, a bit like a tyre that has gone slightly soft under load. Nothing has burst. A disc herniation is when some of the soft inner material pushes through a weak point or a tear in the outer ring. Radiologists grade this further as a protrusion, an extrusion or a sequestration depending on how far the material has travelled, but for a patient the practical question is simpler: is anything pressing on a nerve, and are your symptoms following that nerve.
The popular phrase “slipped disc” is a misnomer. Discs are firmly attached top and bottom and do not slip. The NHS still uses the term “slipped disc” as a catch-all because it is familiar, but what is actually happening is a bulge or a herniation.
Why the words on your report scare you more than they should
Here is the part that surprises most people. Disc bulges and degeneration are so common in pain-free spines that they are closer to grey hair than to disease. A large systematic review of imaging in people with no symptoms at all found that disc bulges were present in 30% of 20-year-olds and 84% of 80-year-olds, and disc degeneration in 37% of 20-year-olds rising to 96% of 80-year-olds (Brinjikji et al, 2015).
Read that again. By your forties, a “bulging disc” on a scan is statistically normal. It does not mean the bulge is the cause of your pain, and it does not predict how much pain you will have. This is why national guidance is cautious about scanning ordinary back pain in the first place. NICE guideline NG59 advises against routine imaging for non-specific low back pain, precisely because the scan often finds something incidental that then gets blamed for the symptoms.
None of this means your pain is imaginary. It means the picture and the person do not always line up, and the picture is the weaker of the two pieces of evidence. We wrote more about that gap in what an MRI report can and cannot tell you.
When a disc problem genuinely matters
A disc finding starts to matter when your symptoms track it. The classic example is sciatica, where a herniation presses on a nerve root and you get pain, pins and needles or weakness running down one leg in a specific band, often past the knee. When the story, the examination and the scan all point at the same nerve, the disc is probably relevant.
It is worth separating this from ordinary mechanical back pain. A lot of back pain has no single structure to blame and is driven by load, stiffness, deconditioning and stress rather than a specific disc. That kind of pain stays mostly in the back and does not send a clear signal down one leg. When there is no leg pain and no nerve signs, a bulge noted on a scan is usually a bystander rather than the culprit, which changes how we treat it.
The reassuring part is that even genuine disc herniations tend to improve with time. The inflamed nerve settles, and the herniated material is often gradually reabsorbed by the body. Most cases of sciatica from a disc improve over a number of weeks to a few months with movement, activity modification and pain control, without surgery. The NHS notes that most back pain, including disc-related pain, improves within weeks. Surgery is reserved for the minority who do not settle or who have significant nerve compression.
Red flags: when to see a GP or A&E urgently
A small number of disc problems are urgent. If you have any of the following, do not wait for a routine appointment, contact a GP urgently or go to A&E:
- Numbness or pins and needles around your back passage, genitals or inner thighs (the “saddle” area).
- Difficulty passing urine, loss of bladder or bowel control, or not being able to feel yourself go.
- Numbness, weakness or pins and needles in both legs rather than one.
- Weakness in a leg or foot that is getting worse, for example a foot that catches or drags.
- Back pain with fever, unexplained weight loss, or pain that is severe at night and not eased by position.
The first two in particular can signal cauda equina syndrome, a rare emergency where a large herniation compresses the bundle of nerves at the base of the spine. It needs same-day assessment to protect bladder, bowel and leg function.
What actually helps a disc problem
For the large majority of disc-related back pain, the evidence-backed approach is unglamorous and effective. Keep moving within tolerable limits rather than resting in bed, which tends to stiffen things and prolong recovery. Stay at or return to work and normal activity as early as you reasonably can. Use simple pain relief if you need it to keep moving.
NICE NG59 supports exercise and movement as the core of treatment, and includes manual therapy, such as the hands-on work an osteopath does, as part of a package that also encourages activity. Manual therapy on its own is not a magic wand, and we would not present it as one. Its job is to reduce guarding and pain enough that you can get back to the movement that does the longer-term work.
What rarely helps is chasing the scan. Repeated imaging, long periods of rest, and treatments aimed at “putting the disc back” all tend to disappoint, because the disc was usually never the whole story.
How we approach it at the clinic
When someone comes in with a disc on their report, the clinic team spends most of the first appointment on the history and a movement and neurological examination, not on the scan. We are checking whether your symptoms genuinely follow a nerve, screening for the red flags above, and working out what you can do today to move more comfortably. If anything points to something that needs a GP or imaging, we say so and refer.
If this sounds like what you are dealing with, an assessment is the next step. Book at hardimanperformance.com/book-online.