
Most musculoskeletal MRI reports tell you less than your symptoms and your movement do. The same disc bulges, joint changes and tendon abnormalities show up in adults with no pain at all. An MRI is essential when specific red flags are present. For ordinary back, neck and joint pain, it usually adds noise to a decision the clinician can already make.
The short version
- Disc bulges, joint wear and tendon changes are common in adults with no pain.
- NICE advises against routine imaging for non-specific back pain.
- MRI matters when red flags are present: progressive weakness, loss of bladder or bowel control, suspected fracture, infection or cancer.
- A scan finding is not automatically the cause of your pain.
- Useful question to ask: would the imaging change my next treatment step?
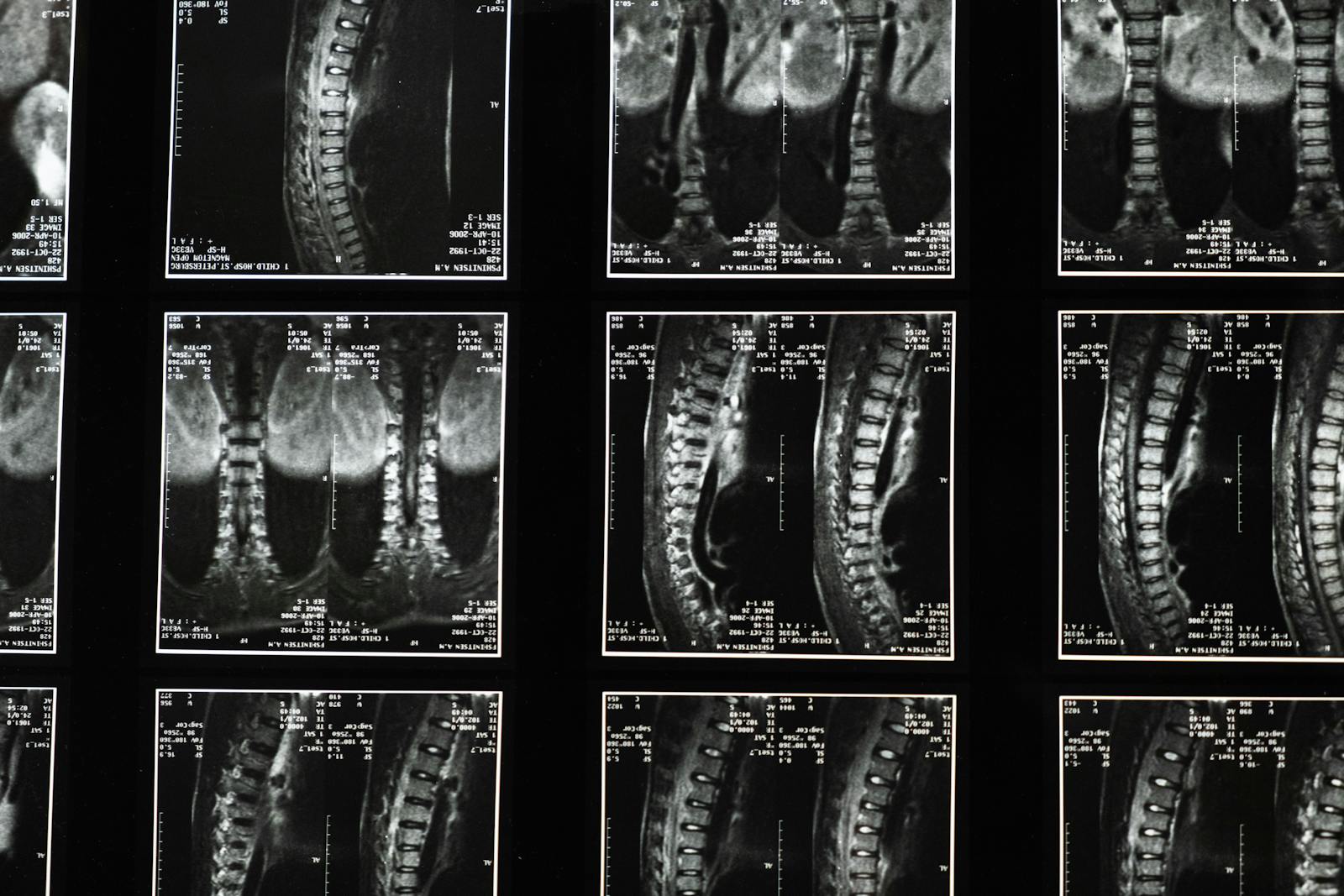
What the scans actually show in people with no pain
The single most cited paper on this is a 2015 review by Brinjikji and colleagues, who pooled data from 33 studies covering more than 3,000 adults with no back pain (Brinjikji et al., 2015, American Journal of Neuroradiology). The numbers are sobering. Disc degeneration on MRI was found in 37% of asymptomatic 20-year-olds and 96% of asymptomatic 80-year-olds. Disc bulges in 30% of 20-year-olds and 84% of 80-year-olds. Annular fissures, facet joint changes, mild spondylolisthesis: all common, all symptom-free.
This is not new science. Jensen and colleagues found the same pattern in the New England Journal of Medicine in 1994: in 98 adults with no back pain, 52% had a disc bulge on lumbar MRI and 27% had a disc protrusion. The body’s spine, like its skin, accumulates marks that have nothing to do with pain. We just rarely look.
If you scanned a sample of pain-free adults today, you would find a meaningful proportion of “abnormal” reports. The reports would be accurate. What they describe exists. They would also be largely irrelevant to whether the person has, or will develop, pain.
Why scan findings can mislead
Three problems sit on top of each other.
First, correlation. A finding on an MRI is not a cause. It is something that happens to be present at the same time as the pain. Some findings genuinely drive symptoms. Many do not. Without a careful clinical match between what the imaging shows and what the patient describes, the report becomes a list of incidental observations dressed up as a diagnosis.
Second, timing. Most degenerative findings pre-date the current episode of pain by years, often decades. A 45-year-old with new back pain whose MRI shows L4-L5 disc degeneration almost certainly had that degeneration five years ago, when they had no pain at all. Pointing at it as “the cause” reads tidy but rarely changes what works.
Third, diagnostic anchoring. Once a patient sees a scary-sounding term on a report, whether “disc protrusion”, “facet arthropathy”, or “tear”, it shapes how they move, what they avoid, and how they describe their pain. The label sticks even when the underlying issue resolves. In my years practising I read a lot of reports that did more damage to the patient’s confidence than the underlying problem did.
When MRI is the right call
This is the part that matters. There is a clear set of situations in which imaging is essential and delaying it is dangerous. NICE guideline NG59 on low back pain and sciatica sets these out for the UK. The decision threshold is whether the imaging would change management.
Imaging is indicated when there are red flags suggesting a serious underlying cause. These include progressive neurological loss (weakness in a leg or arm that is getting worse), loss of bladder or bowel control, saddle anaesthesia, suspected spinal fracture (especially in older adults or after significant trauma), suspected infection (fever, night sweats, unexplained weight loss alongside pain), or suspected cancer (previous history of cancer, persistent night pain, severe systemic symptoms).
If any of those features are present, imaging is not optional. Talk to your GP urgently or go to A&E. The NHS pathways for these scenarios exist precisely because the consequences of missing them are serious.
Imaging is also useful when surgical planning is on the table, or when conservative care has been given a fair trial (typically several weeks to a few months for non-specific pain) and is not delivering, and the next step is a more targeted intervention that depends on knowing the specific anatomy.
When MRI tends to be the wrong call
The cases I saw most often where imaging was driving anxiety without changing the plan looked like this: a few weeks of new back pain in an otherwise well adult, no red flags, a scan requested either by the patient or by a clinician under pressure, a report full of degenerative findings, and a patient now convinced their spine is falling apart. The treatment plan would have been the same with or without the imaging: load management, movement, time, reassessment.
NICE is explicit on this. The guideline recommends against routinely offering imaging in non-specialist settings for people with low back pain with or without sciatica. The reason is that in the absence of red flags, the findings are highly likely to be incidental, and acting on them tends to lead to more interventions, more anxiety, and worse outcomes than not scanning.
The NHS guidance on back pain mirrors this. The starting point is not a scan. The starting point is movement, time, and reassessment if pain is not settling.
What a clinician should be doing instead
The clinical work that replaces the imaging is unfashionable but more useful. A careful history covering what changed before the pain started, what makes it better or worse, what other systems are involved. A movement assessment that reproduces or modifies the pain. A neurological screen if relevant. A trial of conservative care with clear markers for what should change and by when. A planned reassessment at a fixed point. Imaging if the trial fails AND the result would change the next step.
This is duller than a scan. It is also more diagnostic in the cases where diagnosis matters most.
If your scan already shows something, what does it mean?
If you have a report in front of you with “disc bulge” or “facet arthropathy” or “mild degeneration” written on it, the most important thing to do is talk to a clinician who will interpret it in the context of your actual symptoms and movement, not the words in isolation. Most of those findings are incidental. Some are not. The difference is in the matching.
It is rarely a good idea to change your activity based on imaging alone. People who reduce movement because of a scan often end up worse, not better, because deconditioning is its own problem and movement is part of recovery for most musculoskeletal pain.
What to ask before you push for a scan
Three questions sort most cases.
Would the result change my treatment? If a clinician would do the same thing whether the scan is normal or abnormal, the scan is not adding information. It is adding cost and anxiety.
Are red flags present? If yes, the scan is not a question. It is a referral.
Have I given conservative care a fair trial? Most non-specific musculoskeletal pain settles meaningfully within six to twelve weeks with appropriate movement, load management and reassessment. If it has not, the imaging conversation is reasonable. If it is week two of a new episode and there are no red flags, it is almost certainly too early.
The MRI is a tool. Like any tool, it is excellent in the cases that need it and unhelpful in the cases that do not. Most of the cases that walk into a clinic do not need it. The cases that do, need it urgently.
If you are dealing with pain that has not settled with appropriate movement and time, the next step is a careful assessment, not a scan. If you are nearby and want one, the clinic team takes new patients via our booking page.