
Most rotator cuff tears in people over 50 are degenerative, the result of gradual tendon wear rather than one injury, and for those the evidence is reassuring: a well-structured rehabilitation programme often does as well as surgery. Surgery still has its place, mainly after a significant traumatic tear or when months of good rehab have not shifted the pain. The difficult part is telling those two situations apart, and that is what an assessment is for.
Cuff tears are one of the most common things the clinic team is asked about, and one of the most over-worried. Here is what actually decides whether a tear needs an operation.
The short version
- Most cuff tears over 50 are degenerative, not a one-off injury.
- For degenerative tears, rehab often matches surgery for pain and function.
- A sudden tear with real weakness after trauma needs a surgical opinion.
- Many cuff tears cause little or no pain at all.
- See a GP urgently if you cannot lift the arm after injury.
What the rotator cuff actually is
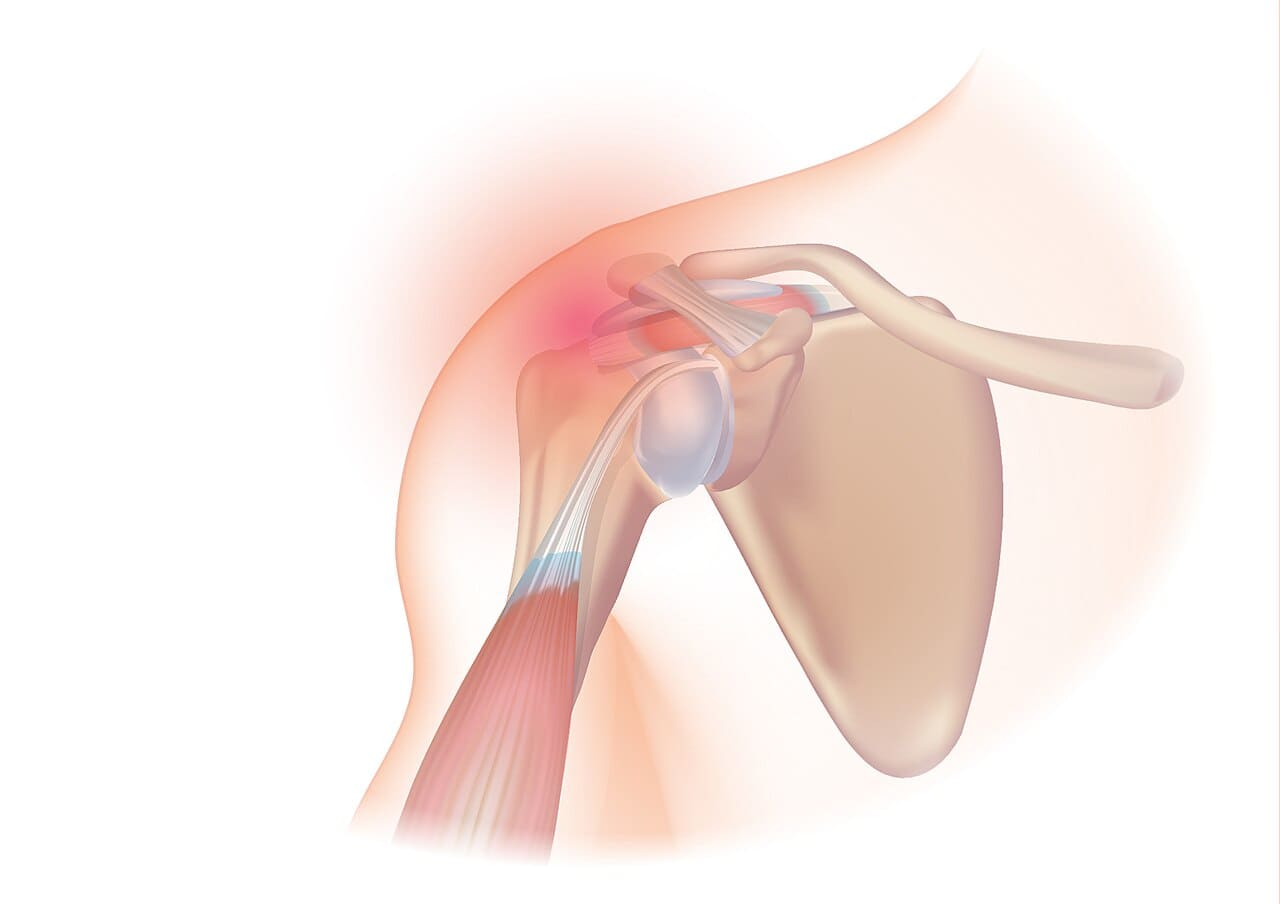
The rotator cuff is a group of four muscles and their tendons that wrap around the top of the arm bone and hold it centred in the shoulder socket. Their job is fine control, keeping the ball of the joint sitting correctly while the bigger muscles do the heavy lifting.
When people talk about a cuff tear they usually mean a tear in one of those tendons, most often the supraspinatus at the top. Rotator cuff related shoulder pain is very common, and the NHS notes that recovering from shoulder pain can take six months or longer. That timeline is often the part patients are least prepared for.
Two kinds of tear, and why it matters
Tears fall into two broad groups, and the group changes the plan. Degenerative tears build up slowly as a tendon ages and its blood supply drops. They are common from the fifties onward, and a good number of them cause little or no pain.
Traumatic tears are different. They happen in a single moment, usually a fall onto the arm or a heavy pull, and they often bring a sudden drop in strength. A traumatic tear in a younger or very active person is the situation where an early surgical opinion earns its place, because a fresh tendon repaired promptly tends to do better than one left for months.
It also helps to know that not every painful shoulder is torn. A lot of shoulder pain comes from irritation and impingement, where the tendons are pinched and sore but intact. And a tear seen on a scan is not automatically the cause of your pain, because cuff tears turn up in plenty of shoulders that feel completely normal. We treat how the shoulder behaves when we test it, not the scan report alone.
What the evidence says about surgery versus rehab
For degenerative tears, the research does not support rushing into an operation. A systematic review and meta-analysis comparing conservative care with surgical repair concluded that a proper rehabilitation programme can give similar results to surgery at short-term follow-up. Where surgery did score better on some one-year measures, the difference was often too small for a patient to actually notice.
A wider synthesis of Cochrane reviews pointed the same way. It found that strengthening exercises, with or without manual therapy, had the greatest treatment effect over the medium and long term for shoulder pain, ahead of surgery and passive options like electrotherapy. None of this means surgery never helps. It means that for the common degenerative tear, loading the tendon properly is a sensible, evidence-backed first choice.
When a tear does need a surgical opinion
Some tears should be seen by a shoulder surgeon sooner rather than later. The main ones are a large traumatic tear, especially in someone younger and active; a sudden and marked loss of strength, such as being unable to hold the arm out to the side; and a tear that has not improved after a genuine three to six month course of well-structured rehab. In our clinical experience these are the minority, but they are the cases where waiting has a cost.
The word genuine is doing a lot of work there. A few weeks of vague stretching is not a fair test of rehab. Building a cuff tendon back to strength takes months of progressive, specific loading, and the decision to consider surgery only makes sense once that has actually been done.
When to see a GP or seek urgent help
Most shoulder pain is not dangerous, but a few signs mean you should get checked promptly rather than manage it alone. See a GP, or use an urgent care service, if you cannot lift or hold the arm after a fall or injury, if the shoulder looks out of shape, or if significant weakness came on suddenly.
Seek same-day advice if the shoulder is hot, red and swollen, if you feel feverish or unwell with it, or if you have night pain alongside unexplained weight loss. New numbness, pins and needles, or weakness spreading down the arm and into the hand also needs checking, as that points to a nerve rather than the cuff. Otherwise, the NHS advises seeing a GP if shoulder pain has not started to improve after about two weeks or keeps disturbing your sleep.
How we approach it at the clinic
When someone comes in with a suspected cuff tear, the clinic team starts with an assessment rather than an assumption. We check how much active strength and range you have lost, whether the pattern fits a degenerative or a traumatic tear, and whether anything in your history flags a need for imaging or a surgical opinion. Most people do not need a scan to begin treatment.
From there the work is graded loading of the cuff and the muscles around the shoulder blade, hands-on treatment to settle pain and restore movement where it helps, and a plan you can keep going with at home. It is not fast, and we will be honest with you about that. Our shoulder pain treatment page explains how we work and what to expect.
If this sounds like what you're dealing with, an assessment is the next step. Book online here.
Image: "Rotator cuff syndrome" by Injurymap, used under CC BY 4.0, via Wikimedia Commons.