
Chronic pain is not a sign of ongoing tissue damage, and it is not “all in your head”. It is the nervous system continuing to produce a pain signal after the original injury has healed, often because the system itself has become more sensitive. That distinction matters, because how you understand your pain changes how you treat it.
The short version
- Pain after about 12 weeks is classed as chronic pain.
- Chronic pain is not always proportional to tissue damage on a scan.
- The nervous system can become more sensitive and keep signalling pain after tissues have healed.
- Around 28 million UK adults live with chronic pain, with about 5.5 million in England disabled by it.
- Movement, sleep, stress, and education tend to help more than long-term painkillers.
What chronic pain actually is
Pain is the nervous system’s alarm. In an acute injury, that alarm is useful. Tissue is damaged, the body protects it, and as healing progresses the pain fades. Chronic pain is what happens when the alarm keeps firing after the tissue has healed, or when no clear tissue damage was ever there to begin with.
The standard threshold is twelve weeks. Pain that persists beyond that window meets the clinical definition of chronic, and is approached differently from acute pain. NICE guideline NG193 sets out the framework UK clinicians use, which centres on assessment, shared decision-making, and a move away from long-term opioids and gabapentinoids for chronic primary pain.
What makes chronic pain confusing for patients is that the pain feels exactly as real as acute pain, because biologically it is. The signal is being produced. The mistake is assuming the intensity of the signal tells you the extent of the damage. That is rarely true once pain has settled into a chronic pattern.
It is not “all in your head”
The “it is in your head” framing has done a lot of damage. Patients who hear it usually interpret it as either “you are imagining this” or “this is your fault”. Neither is what the science actually says.
Pain is always produced by the brain. That is true of stubbing your toe, of post-surgical pain, and of chronic back pain. The brain weighs inputs from the tissues, the nervous system, prior experience, expectation, and context, and produces a pain output. In acute injury, the tissue input dominates. In chronic pain, the other inputs often carry more weight than the tissue itself.
That does not mean the pain is imaginary. It means the nervous system has changed. The technical term is central sensitisation, described in detail by Clifford Woolf’s 2011 review in the journal Pain. In central sensitisation, neurons in the spinal cord and brain become more excitable. Normal sensory input gets amplified. Light touch can register as painful. Pain can spread beyond the original site. Movements that would have been comfortable become threatening.
It is not “just damage” either
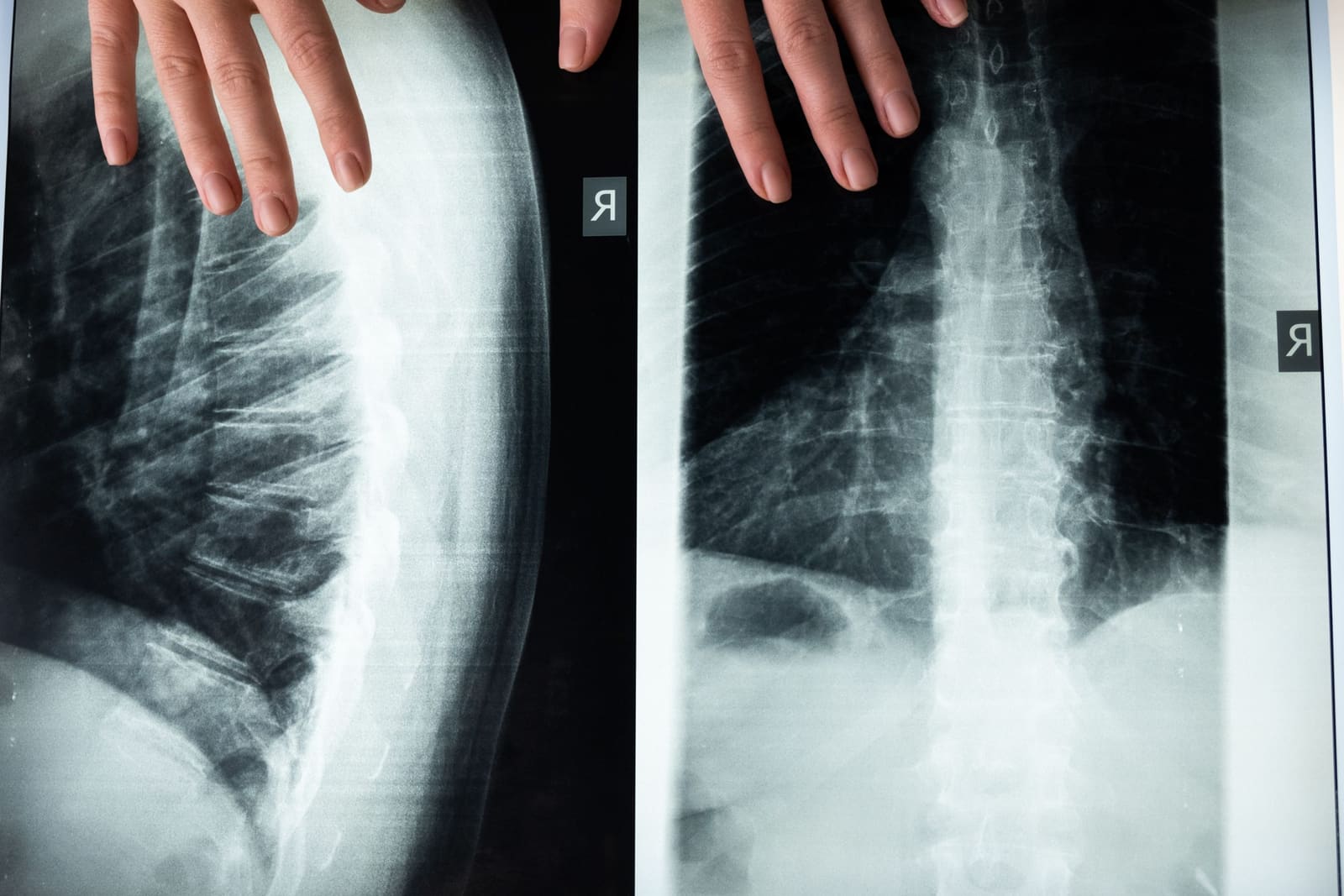
The other common framing is that chronic pain means something is structurally broken and must be repaired before the pain will resolve. Scans are then ordered, findings are reported, and patients are often told their disc, joint, or tendon is the cause.
The problem is that MRI findings and pain do not correlate as tightly as people assume. Disc bulges, degeneration, and arthritic changes show up routinely on scans of people who have no pain at all. Conversely, plenty of patients in severe chronic pain have unremarkable imaging. The structure on the scan is a snapshot, not a diagnosis.
This is why NICE NG193 explicitly recommends against routinely offering imaging for chronic primary pain unless a specific red-flag pathology is suspected. The scan rarely changes what helps. Treating the person tends to outperform treating the picture.
How the nervous system gets stuck
Several things push a healing system toward chronic pain rather than away from it. None of them are character flaws. They are biology.
Poor sleep. Sleep is when the nervous system recalibrates. People in chronic pain often sleep badly, and bad sleep amplifies pain the next day. The loop reinforces itself. NHS guidance places sleep alongside movement as one of the most consistently useful levers.
Avoiding movement. When a movement hurts, the natural response is to stop doing it. In the short term, that is sensible. In the long term, avoidance shrinks the range of pain-free activity. The nervous system, which uses movement as evidence that the body is safe, gets less of that evidence over time. The threshold for what triggers pain drops.
Stress and threat. The same nervous system that processes pain also processes psychological threat. Financial stress, job stress, grief, and anxiety all measurably influence pain perception. This is not weakness. It is shared neural circuitry.
Repeated unhelpful messages. Patients told their back is “crumbling” or that they have “the spine of an 80-year-old” rarely improve faster for hearing it. Words shape expectation, and expectation shapes pain. This is why how a clinician talks about your scan or your prognosis matters as much as what they do with their hands.
What tends to help
The evidence base for chronic pain is not glamorous. There is no single intervention with strong, durable effects across the board. What works is a combination of things, applied consistently, over months rather than weeks.
Graded movement. The goal is not to push through pain, and it is not to wait for pain to disappear before moving. It is to find a level of activity the system can tolerate, then build from there. Walking is usually the easiest place to start. Strength work is added once tolerance allows.
Education about pain. Understanding that hurt does not always mean harm shifts how patients respond to flare-ups. Pain neuroscience education is one of the more researched approaches, with a 2019 systematic review in the European Journal of Pain finding moderate evidence that adding it to standard physiotherapy improves disability in the short term for chronic low back pain. The long-term data is weaker, but the short-term shift in behaviour is worth having.
Sleep and stress management. Not because these are root causes in every case, but because they reduce the background load on the nervous system. A system that is rested and not in constant fight-or-flight has more capacity to recalibrate.
Hands-on treatment, used appropriately. Manual therapy, including osteopathy, has a useful role in chronic pain when it is part of a broader plan that also includes movement and education. As a standalone, repeated indefinitely, it tends to underdeliver. The clinic team’s view is that hands-on work is best used to give a patient a window of reduced pain in which they can do the movement and rebuild capacity. It is not a long-term substitute for that.
Realistic timelines. Acute injuries resolve in weeks. Chronic pain typically improves over months. Patients who expect a six-session resolution usually feel let down. Patients who expect a six-to-twelve month arc tend to make steadier progress, with fewer setbacks pulling them off the plan.
How common is it
Chronic pain is one of the most common health problems in the UK and one of the least well treated. Versus Arthritis estimates around 28 million UK adults live with chronic pain. About 5.5 million people in England have high-impact chronic pain, meaning pain that limits their day-to-day activity. It is more common in women, older adults, and people experiencing deprivation.
If you have been in pain for more than twelve weeks, you are in a large group with a wide range of treatment options. You are not stuck.
When to see a GP rather than continue self-managing
Most chronic musculoskeletal pain is not a medical emergency, but a few patterns warrant a same-day or urgent GP review:
- New numbness, pins and needles, or weakness in a limb that does not settle
- Loss of bladder or bowel control, or numbness around the saddle area (this can indicate cauda equina syndrome and is an A&E presentation)
- Pain that is severe at night and wakes you regularly, alongside unexplained weight loss, fever, or feeling generally unwell
- A history of cancer with new persistent bone pain
- Pain following a significant trauma you have not had assessed
For everything else, NHS advice is to start with your GP, who can rule out red flags, discuss management options, and refer on if needed.
Where osteopathy fits
Osteopathy is one piece of the chronic pain picture, not the whole picture. A useful first appointment looks for the patterns of movement, load, and habit that are keeping the nervous system on high alert, treats with hands-on work where that helps, and gives the patient a clear set of things to do between sessions. If the pain is responding, sessions space out. If it is not, the plan changes, including knowing when to refer on rather than keep treating.
The evidence for manual therapy in chronic pain is mixed and most useful when combined with active rehabilitation rather than offered as a standalone treatment. We are honest about that with patients, because it shapes how the course of care is structured.
If you have been dealing with pain for more than twelve weeks and want an assessment that takes the whole picture seriously, you can book at hardimanperformance.com/book-online. Initial assessment is £75, follow-ups £60.